
Microscopic Lumbar Discectomy
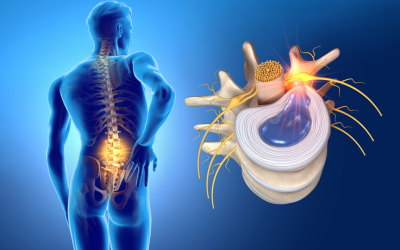
A lumbar disc herniation can greatly affect daily life. It commonly causes pain that begins in the lower back or buttock and travels down one leg, often with burning, tingling, or electric shock-like sensations. This nerve compression may lead to sciatica, numbness, weakness in the leg or foot, and difficulty sitting, standing, walking, or sleeping comfortably.
Most patients improve with medications, physiotherapy, lifestyle modification, and selective injections. However, when pain persists despite conservative treatment, or when there is significant weakness or nerve compression, surgery may be advised. Microscopic lumbar discectomy is a minimally invasive procedure that removes the offending disc fragment, relieves nerve pressure, and helps patients return to normal activity faster.

Dr. Arvind M. Umarani, a highly qualified and trained orthopedic spine surgeon, explains, “Microscopic discectomy is most effective when clearly indicated and precisely performed. Targeted nerve decompression with minimal disruption to surrounding tissue ensures optimal results and lasting recovery.”
Dr. Arvind M. Umarani specializes in minimally invasive spine surgery. His approach to microscopic lumbar discectomy is precision-led, using operative microscope to achieve accurate nerve decompression through a small incision, without damaging the muscles and bone around the affected level. Patients managed under his care for spinal disc surgery benefit from shorter hospital stays, less post-operative pain, and a structured, monitored recovery pathway.
Is your back pain pointing to a disc problem? Let’s look at the key causes and symptoms that indicate lumbar disc conditions.
Causes and Symptoms of Lumbar Disc Problems
Lumbar disc problems often develop gradually over time, although symptoms may also appear suddenly after heavy lifting, bending, twisting, or strain. Early recognition of the cause and symptoms is important, as timely treatment can help relieve pain, protect nerve function, and reduce the risk of long-term complications or more complex treatment later.

Common Causes
Common Symptoms
The Microscopic Lumbar Discectomy Procedure Explained
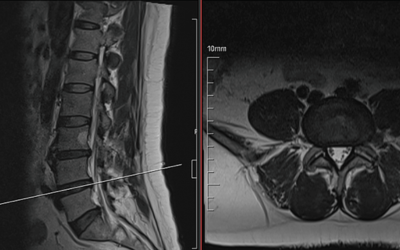
1. Pre-Operative Assessment
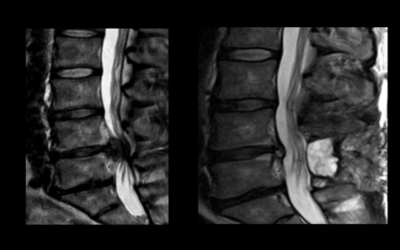
MRI and CT scan findings are carefully correlated with a detailed clinical examination. The affected disc level is confirmed, neurological function is documented, and overall surgical fitness is assessed. The patient’s previous conservative treatment history is also reviewed before deciding whether surgery is necessary.

2. Anesthesia and Positioning
3. Skin Incision and Muscle Retraction
4. Operating Microscope and Bone Work
Dr. Arvind Umarani utilizes the operating microscope for high magnification and illumination of the surgical field. A small portion of the lamina is removed to expose the compressed nerve root and herniated disc fragment, with bone removal kept to the minimum necessary.
5. Nerve Root Identification and Protection
6. Disc Fragment Removal (Discectomy)
7. Confirmation and Closure
Conditions Treated with Microscopic Lumbar Discectomy
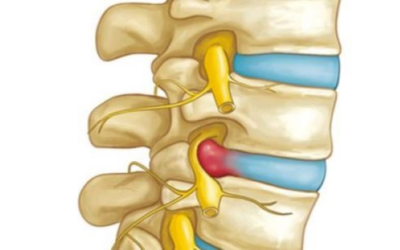
Lumbar Disc Herniation
A herniated disc pressing on a nerve root, causing leg pain, numbness, or weakness, unresponsive to conservative treatment.
Sciatica from Disc Compression:
Disc herniation at L4-L5 or L5-S1 compressing the sciatic nerve, producing radiating leg pain.

Lumbar Radiculopathy
Disc-related nerve root compression causing pain, tingling, or numbness along a specific leg distribution.
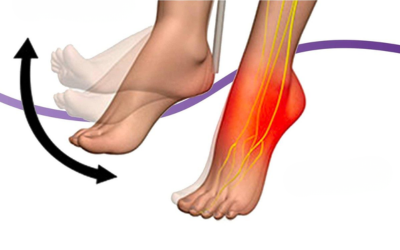
Foot Drop
L4 or L5 nerve compression from a herniated disc causing inability to lift the front of the foot. Early surgery offers the best neurological recovery.
Cauda Equina Syndrome
Large central disc herniation compressing multiple nerve roots and causing bladder or bowel dysfunction. Surgical emergency.
Far Lateral Disc Herniation
Disc material herniated outside the spinal canal, compressing the exiting nerve root at the foramen.

Sequestrated Disc Fragment
A separated disc fragment migrating within the spinal canal, causing significant nerve compression.
Recurrent Disc Herniation:
Re-herniation at a previously operated level causing recurrent symptoms, where revision discectomy may be appropriate.
Why Microscopic Lumbar Discectomy is the Preferred Choice?
High Magnification and Precision:
Muscle-Sparing Approach:
Short Hospital Stay:
Preserves Spinal Stability:
Smaller Incision:
Faster Return to Activity:
Proven High Success Rate:
Lower Complication Rate:
Why Choose Dr. Arvind Umarani for Microscopic Lumbar Discectomy?
Fellowship-Trained in MIS Spine Surgery
International Training in Advanced Techniques
Conservative First Approach
 | drarvindumarani.in")
Clear Communication Throughout
Structured Post-Operative Care
Handles Complex and Revision Cases
Frequently Asked Questions
1. What is a microscopic lumbar discectomy, and how is it different from open disc surgery?
2. When is a microscopic lumbar discectomy recommended over conservative treatment?
3. What is the success rate of microscopic lumbar discectomy?
4. When will I be able to walk after surgery?
5. What is the recovery time after a microscopic lumbar discectomy?
Disclaimer: The information shared in this content is for educational purposes and not for promotional use.